|
NOTE: Some of the the following sections are complex, and involve information which many doctors do not know! You do not have to read it all!
|
Injection Treatment of
Spider Veins
by Ken Biegeleisen, M.D.
|
NOTE: Some of the the following sections are complex, and involve information which many doctors do not know! You do not have to read it all!
|
TABLE OF CONTENTS
| I. | |
|
II. |
|
|
|
|
|
III. |
|
|
IV. |
|
|
V. |
|
|
VI. |
|
|
VII. |
|
|
VIII. |
|
|
IX. |
|
|
X. |
|
|
XI. |
![]()
Injection Treatment of Spider Veins
by Ken Biegeleisen, M.D.
|
Before even beginning this discussion, let's get our terminology straight. When I was in medical school, they taught me that a "spider vein" (or, more accurately, "spider angioma") was a little star-burst pattern of blood vessels on the chest of a patient who was dying of liver disease. Obviously, this has nothing to do with cosmetic problems of the legs! In other words, those unsightly blood vessels which haunt the legs of most American women are not really "spider veins". But what is their name? The answer is: they have no name! There's a "class" name, of a general nature, which is used for a large variety of abnormally enlarged blood vessels of various sorts, and on various body parts: telangiectasia. It is therefore entirely accurate to refer to tiny, unsightly leg veins as "telangiectasias of the legs", or "lower extremity telangiectasias". Unfortunately, however, the term "spider veins" for leg veins has become so widespread that it's almost impossible to not use it! It is universally in use among patients, and even among the majority of doctors. In articles in women's magazines, the use of the term "spider veins" is inevitable. Therefore, although there is technically no such thing as a "spider vein" of the legs, the term is so widely used these days that we shall stick to it ourselves, as a matter of pure expedience. |
|
II. What causes "spider veins" (of the legs)? a. Elevated pressure from "arteriovenous communications". WARNING! The following discussion is highly technical, and no attempt has been made to "abridge" it. It represents my own best effort to explain spider veins. It is a theory, and is not proven (there is no universally-accepted explanation for spider veins at this time). If you hate long, drawn-out scientific discussions, please skip ahead to the next subject. If you get through all of the following discussion, you'll know more than most doctors! If you're still reading, the drawing below shows spider veins on the outside of the thigh. This pattern, a fan-shaped array, is, without a doubt, the most common pattern seen: |
|
|
|
The vessels which form the fan-shaped array are small, usually ranging in diameter from 1 millimeter down to 1/10 millimeter (less than 1/50 of an inch). Note, in the drawing above, that there is a larger vessel, extending from the knee toward the fan-shaped array of small vessels. This larger vessel is called a "reticular" varicose vein. We will discuss these later. In case you don't have spider veins yourself, or if my drawing above does not make it absolutely clear what we're talking about, here is a photo of an actual patient. I hope you will agree that my poor "artist's interpretation" above is a reasonable representation of this:
Spider veins always occur in groupings, such as the one depicted above. There are others as well. All together, there are six such groupings which are commonly seen. Three of them are on the outside of the leg. Here they are: |
|
|
|
As mentioned above, the most common pattern is the fan-shaped array on the outside of the thigh (labeled "1" in this drawing). Then there's a second fan-shaped array located just below the knee ("2"), and one on the outside of the ankle ("3"). For each of these three groups of vessels on the outside of the leg, there is a similar grouping of vessels on the inside of the leg (not shown in the drawing), giving a total of 6 groups in all; three on the outside (shown above) and three on the inside. And just what is a spider vein? Many people mistakenly think that spider veins are "baby" varicose veins, destined to grow ever larger and larger. They are not. Here are some differences: |
|
|
Varicose veins, most of the time, are |
|
|
|
|
|
|
|
|
Spider veins, most of the time, are |
|
|
|
|
The cause of spider veins is not known. When I first went into medical practice, in 1979, the talk among doctors concerning the cause of spider veins was positively ridiculous. Patients were told things like "spider veins are caused by too much sunlight". Hey, that's not true! Besides, even if it were true, that's still not an explanation. Just how would sunlight cause spider veins, anyway?! A better explanation was offered by myself in 1983, when I delivered a paper on "The Physiology of Lower Extremity Telangiectasias" at the World Congress of Phlebology at Brussels. As far as I know, it was the first paper ever written on the subject of what actually causes spider veins of the legs. It was eventually published in the American journal Angiology (Volume 38, October 1987, pp. 760-768) under the title "Primary Lower Extremity Telangiectasias -- Relationship of Size to Color". In the article, I proposed that leg spider veins were the results of arteriovenous communications. In order to understand what an arteriovenous communication is, you first must refresh your memory about the physiology of basic circulation (or, if you've had just about as much physiology as you can stand, click here to move ahead!). Please take a look at this simple drawing: |
|
|
|
Recall that the heart pumps blood into arteries (labeled "A"), which are thick-walled, high-pressure vessels. Because the arteries bear the brunt of the blood pressure, they are endowed with thick muscular walls, capable of withstanding these high pressures. Next, the blood is dispersed into tiny capillaries ("C"). Although the drawing shows only a few capillaries, that is an artistic expedient. Actually, the body is packed, from head to foot, with countless billions of capillaries, which fill every available space. Have you ever tried to breathe through a straw? It's difficult. How about a small straw, like a cocktail straw? It's more difficult still. Now imagine how much work it would take to pump your blood through a billion capillaries -- vessels which are so small that they can't be seen without a microscope. Believe me, it's hard. Consequently, when the blood collects on the vein side (i.e., venous side) of the circulation ("V" in the drawing above), there's very little pressure remaining. Most of the pressure was used up in the trip through the capillaries. Let's throw some numbers in. "Blood pressure", as the term is commonly used, means arterial blood pressure. This is what your doctor measures when he puts that tight cuff on your arm. Doctors don't routinely measure the pressure in veins. This latter pressure, the so-called venous pressure, can only be measured in specially-equipped laboratories. If you pay attention to your own blood pressure, then you are familiar with numbers such as "120 over 80". This means that when the heart beats, there's a pressure of 120, and when the heart relaxes, between beats, the pressure only drops to 80 -- not zero. Therefore, the average blood pressure (in your arteries), at any moment, is midway between the two, i.e., about 100. That's arteries. What about veins? It turns out that the so-called venous pressure is variable, depending on which part of the body we're talking about, and what the position of the body is. On the average, the venous pressure is about 10! This means that the arterial blood pressure is ten times higher than the venous pressure! We may now ask a question: What would happen if arterial blood, with a pressure of 100, got into a vein, without first passing through a capillary? Well, in that case, the blood pressure in the vein would rise from 10 to 100. Since veins have thin walls, with much less muscle than thick-walled arteries, the vein might be expected to blow up, like a balloon. That, in fact, is precisely what happens. This is easiest to see in a particular man-made situation where arteries and veins are intentionally crossed. This situation occurs in those unfortunate people who have total kidney failure, and need to have their blood filtered (called dialysis) to stay alive. In order to filter a person's entire blood volume, you need access to a large blood vessel, at least twice a week. But there are no vessels on the surface of the human body which are large enough. So the surgeons have to make one! They do this by opening up the wrist, and finding a small artery inside. (Remember, an artery is a high-pressure vessel). Then they connect it to a small surface vein on the arm. Now all the arterial pressure is transferred to the surface vein. Voila! In no time at all, the surface vein blows up like a balloon! So the transmission of arterial pressure to a vein does make the vein enlarge. But does this have anything to do with spider veins? I think that it does, and I have been saying so since 1983. It has been discovered that skin circulation doesn't follow the general rule of: |
|
|
|
Rather, in the skin, there are large numbers of blood vessel networks which contain no capillaries: |
|
|
|
In these pathways, it is possible for blood to be pumped from the arteries directly to the veins, without passing through billions of capillaries. I said "possible" because these pathways are usually closed off, by a ring of muscle called a "sphincter". The sphincter only opens up in response to certain types of neurological stimulation. There are at least two circumstances known where these sphincters will open up. One such circumstance is when you blush. If you are embarrassed, your brain sends a message to millions of such sphincters in your face, which then open up. This allows relatively huge amounts of blood to flood into the veins adjacent to the sphincters, filling your skin with extra blood. Then your face "turns red"! The other circumstance which is well-known is the circumstance where you are overheated, such as after running a mile on a hot summer day. Your entire body, under such circumstances, will be flushed and red, because of the opening up of these sphincters. Why does your body do this? Because the skin temperature is considerably lower than your internal body temperature of 98.6° . By dumping lots of hot blood into the skin, your body is able to get rid of excess heat, which radiates out from the skin into the surrounding air. Therefore, the primary (known) purpose of these pathways of circulation is temperature regulation. These are circulatory pathways which are usually closed, but which open up when your body is overheated, to allow excess heat to radiate from your blood, out into the surrounding air. Each of these temperature-regulating pathways consist of arteries and veins, but no intervening capillaries. Let us now ask how many such vessels there are in the skin. Research by circulatory physiologists has revealed the surprising fact that most of the blood vessels in the skin (at least 80%) are there for only one reason: temperature regulation! This is an astonishing fact for someone who has been taught in school that circulation is nutritional, i.e. for the purpose of delivering oxygen and food to our cells. But all delivery of oxygen and nutrients occurs through the walls of microscopic capillaries. No oxygen or nutrients can get through the relatively heavy walls of either arteries or veins. Therefore, what we are saying is that at least 80% of the blood vessels in the skin have nothing to do with nutrition! They are part of a vast network of pathways which consist of arteries and veins, without capillaries in between them. These pathways are usually closed; opening up only when the body is overheated (or when you blush). What does this have to do with spider veins? It turns out that spider veins may not be a vascular disease at all, but rather a disorder of those sphincters which we have just discussed. What would happen if one or more of those sphincters became constantly open? The veins on the other side would then have constant arterial blood pressure. Remember that the arterial pressure is higher than the venous pressure. So now, instead of being exposed to arterial pressure only when you blush, or when your body is overheated, these veins are exposed to arterial pressure constantly. They are not built to withstand this! As the months and years go by, they gradually stretch and thicken. After a while, they get so large that you can see them. You don't like what you see! This entire scenario is a theory, but it is abundantly supported by evidence. The color of blood is well-known to reflect the oxygen content, and the color of spider vein blood is usually purple; sometimes cherry-red. This indicates high oxygen content, something normally found only in arterial blood. In contrast, vein blood looks blue, when viewed through the skin. Look at the veins on the back of your hand -- they're definitely blue, not red. It is therefore a certainty that there is arterial blood in spider veins. Furthermore, the fact that the doctor can inject relatively large amounts of medicine into the spider veins proves that they are not part of the nutritional circulation. If they were, the treatment would be expected to produce damage to the skin by interfering with its normal circulation. In actual fact, skin damage occurs only as a result of mishaps, and never as a normal treatment outcome. Even in patients who have had maintenance treatment for spider veins over a lifetime (my father treated patients from 1926 to 1975, nearly 50 years), there is never any harm to the skin. The above theory is the single best explanation I can offer for spider veins, based on the information currently available. Again, this theory states that your body loses control over one or more sphincters in the temperature-regulating networks of blood vessels, resulting in the sphincters becoming open all the time. The veins attached to those sphincters are then exposed to constant arterial blood pressure, causing them to gradually dilate and become unsightly. |
|
What causes "spider veins"? b. Low-grade underlying varicose veins Having said all the above, regarding the theory of spider veins arising from arteriovenous communications, I must now inform you that there is a second plausible theory of causation of spider veins. I first learned of it through the Phlebologists (i.e., vein specialists) of France, whose capital city, Paris, has more distinguished vein injection specialists than any other city I know of. The following, by the way, is another discussion you may wish to skip if you hate technical talk (click here to move ahead). I'd suggest that you try to read it, but don't be concerned if you don't understand it all. Remember, most doctors don't know these things! In the late 1980's, the French Phlebologists, and their American disciples, began proposing that all spider veins were "end branches" of varicosities of the greater and lesser saphenous veins. (If you are not familiar with varicose veins in general, or with the saphenous veins in particular, please return to the Home Page of this Web Site, and follow links for "Varicose Veins", or else go directly to our informative write-up on this subject, entitled "Injection Treatment of the Greater Saphenous Vein".) The French theory states that all patients with spider veins on the insides of their legs have varicose veins involving the underlying greater saphenous vein, a relatively large vein which runs the length of the leg, from the groin to the ankle. Spider veins on the outside of the leg - they say - arise from the lesser saphenous vein, which runs down the back of the leg from the knee to the heel. The French theory is based upon the well-established fact that the saphenous veins, when they become varicose, have elevated pressures (venous pressures; not to be confused with common "hypertension"). These elevated venous pressures are transmitted into the many branches of the saphenous veins, and from there to tiny microscopic veins in the skin. The elevated pressures cause the skin veins to enlarge, until they become visible and unsightly. This theory suggests that the "key" to a fast and effective removal of spider veins is an aggressive attempt to eliminate the underlying varicose veins. But there's a problem: most patients with spider veins do not seem to have underlying varicose veins! Because of this obvious contradiction, we were, for several years, skeptical of the French theory. However, after we began doing routine ultrasound studies on spider vein patients, we found occasional cases where the underlying saphenous veins were grossly diseased (i.e., varicose). In one particular case, which was a turning point in our own office, a woman with what were previously intractable (i.e., incurable) spider veins of the inside of her calf was completely cured after treatment of an underlying greater saphenous vein which was discovered, on routine ultrasound study, to be severely varicose! Subsequently, we discovered many other similar cases. We therefore now acknowledge that elimination of grossly varicose veins is essential to the management of spider veins in the skin above. But the fact still remains: most spider vein patients do not have demonstrable varicose veins! (Not even on ultrasound examination). Cases like the one mentioned above are in the minority. Furthermore, there's a widespread opinion among certain vascular surgeons that the saphenous veins should be saved for coronary artery bypass. Please see our write-up on the saphenous veins for a full discussion of this subject. When the saphenous veins of the average spider vein patient are studied by ultrasound, they are usually found to be larger than normal, but only slightly so. There is a suggestion of abnormal blood flow, but only that: a suggestion. There is, as a rule, no grossly demonstrable abnormal flow. What does this mean? One of two things: It could mean that these veins are truly abnormal, but that our machines are not sensitive enough to detect it. Or, it could mean that these veins are not really abnormal, and that the suggestive evidence seen on the ultrasound studies is merely an artifact of some sort, totally irrelevant to health. We have no way of knowing! Because of this uncertainty, there is a division of opinion concerning the proper way to deal with the saphenous veins in spider vein cases. A minority of aggressive physicians inject ALL saphenous veins before even approaching the spider veins. These doctors are assuming that the saphenous veins are all abnormal, whether or not ultrasound shows it. Therefore they ignore ultrasound entirely, and treat all saphenous veins as "the enemy". Most practitioners of spider vein injections, however, do not treat the saphenous veins at all. This is because of the odd (and, in my opinion, aberrant) situation that most spider vein injectors, these days, are unqualified amateurs who have no vascular training, and who wouldn't dare put a needle into any vein larger than a strand of uncooked spaghetti. In our office, we take a middle position. All grossly abnormal saphenous veins are treated (with the patient's consent, of course). Saphenous veins which cannot be shown to be grossly abnormal are left alone, unless the overlying spider veins prove to be difficult or impossible to remove. In that case, we may advise treatment of the underlying saphenous veins, which usually brings about a successful conclusion to the spider vein treatment. |
|
What causes "spider veins"? c. "Popular" theories (birth control pills, etc.) Now that you know how complicated spider veins really are, you will perhaps understand that they cannot be rooted out by any simple procedure, such as taking some sort of medicine by mouth. Nevertheless, some people still think that spider veins have more simple causes than those I have discussed above. No, "the sun" does not cause spider veins! But what about things like birth control pills? Or exercise? One well-known researcher has published a computerized statistical study which supposedly shows that a person's lifetime total exposure to birth control pills and other estrogens determines how bad their spider veins will be. I cannot validate this theory by my own observations. Furthermore, I'm not sure how it relates to men, who also get spider veins. For many years, when I took general medical histories of my spider vein patients, I specifically asked detailed questions about birth control pills. When patients had been on "the pill" in the past, these were my observations: There were very few patients who reported that their spider veins started when they began taking birth control pills. In most cases, the veins had started years before they had gone on "the pill", or years after they went off it. Furthermore, few patients with spider veins who had been on the pill reported noticing any worsening of their cases during the time that they were on it. Nor did any patients report an improvement in their veins when they went off it. Therefore, based on my own observations, I find no conclusive evidence that birth control pills have a significant effect on spider veins. Accordingly, I cannot recommend going off birth control pills, if the purpose of going off is to prevent spider veins. There may be other reasons for going off the pill, but they are beyond the scope of this discussion. |
|
d. Exercise I also find no evidence that exercise either causes or cures spider veins. If my memory is to be trusted, I cannot recall a single case of a woman reporting that the onset of her spider veins was at the time she began an exercise program. The "women's press" is prone to publish misleading articles about the relationships between exercise and veins. Years ago, when Jane-Fonda-like "high-impact" aerobics was popular, the women's magazines often featured articles purporting to show that various vein problems were due to lack of exercise. No evidence was presented; only opinions. When "high-impact" fell out of favor, and "low-impact" aerobics became popular, some of the very same magazines ran new stories, now purporting to show that the same vein problems were caused by too much exercise! Again, there was no evidence presented; only opinions. It's my opinion that exercise has no effect whatsoever on spider veins. The effect of exercise on large varicose veins is more difficult to assess. Please see our write-up on the saphenous veins for more on that. |
|
e. Trauma Through the years, many patients have claimed that their spider veins were the result of an injury. The trouble is, most of them had the veins on both legs, whereas the injury was only on one leg! Obviously, there's something wrong with that theory! In spite of this, I have seen a few patients who have spider veins which certainly do seem to be the result of injury. They are localized to a single area -- the area which was injured. The affected area usually contains a multitude of closely-packed, tiny red vessels. These are difficult or impossible to inject away. Such trauma-induced spider veins are not very common, and they're not something that the average patient has to worry about. Similarly, spider veins can, on occasion, appear after surgery (a form of controlled trauma), especially cancer surgery. These, too, are difficult or impossible to inject away. Again, this is not something that the average spider vein patient has to worry about. |
|
III. What treatments exist for spider veins? There's only one treatment for spider veins: injections. What about laser? You've surely seen all the advertisements, magazine articles and television shows, which, for nearly 20 years, have been promoting laser as a "miracle" treatment for spider veins. Well, it doesn't work! If you wish to read the dismal history of the attempts to manage spider veins by laser, click HERE. Otherwise, the remainder of this discussion will be about injections. If you followed the long, drawn-out discussion about what causes spider veins, then you know that regardless of what causes them (i.e., whether they are caused by arteriovenous communications, or by low-grade varicose veins), they are a surface manifestation of a deeper problem. In other words, the unsightly vessels on the surface are not, themselves, a disease. They are caused by a problem which is deeper in the leg, where we cannot see. The nature of the problem, as you have seen, is rather complicated, and it is far from fully understood by doctors. When we know (mainly from ultrasound studies) that varicose veins are contributing to spider veins in the skin above them, we begin our treatment by treating the underlying varicose veins. This usually "knocks the stuffing" out of the spider veins above, as their source of abnormal blood flow is thereby cut off. Then they respond very quickly to routine surface injections. In other cases, however, we cannot find any varicose veins beneath the spider veins. This, in fact, is the usual case. Then we have a more difficult problem. We presume, then, that the spider veins are mainly the result of arteriovenous communications. The trouble is, we can't see the arteriovenous communications, because they are very small, and they are hidden beneath the skin. Also, there are NO TESTS (i.e., x-rays, etc.) which can reveal to us exactly where they are. We're in the dark! The only recourse we have in most of our cases is, therefore, to inject the visible veins on the surface. Since patients have many spider veins, the treatment takes many injections. This is not really a very "clever" treatment, but it's the only one we have. Here's how it goes. |
|
|
|
The above drawing will be referred to repeatedly throughout the following discussion. This is one of the most important pieces of information you will receive in this write-up, and you should make certain that you understand it. Drawing "A" shows, once again, that fan-shaped array of vessels on the outside of the thigh. As we said earlier, this is the most common pattern of spider veins. What happens to these vessels after they are injected? After the first treatment, most (or all) of these unsightly vessels will have received medicine, and will therefore disappear (they actually take a month or two to shrink, but I have taken the liberty of not including them in the other drawings). But even after these initial, or primary vessels are completely gone, the area will NOT be clear! Why not? Because they are replaced -- replaced by a second set of vessels, different from the primary ones! We therefore call these new vessels "secondary vessels". What do they look like? I've attempted to indicate this in drawing "B" above. Here are some characteristics of these "secondary vessels", as depicted schematically in drawing "B":
Although the secondary vessels are generally less unsightly than the original primary vessels were, they still need to be treated. The treatment at this point becomes difficult, and requires an expert. Your local dermatologist will not be able to handle them! To see how the treatment progresses subsequently, please refer back to our illustration, reproduced here, and slightly enlarged:
What these drawings attempt to show is that each successive treatment breaks up the vessels into smaller and smaller size, scattering them like a shattered glass. The net result is a "thinning out" effect, which continues until the treatment is over. Thus, in drawing "D", nothing remains except tiny vessels, and these are scattered about the general area. At this stage, one additional "going over" brings the treatment to a conclusion (drawing "E"). This set of drawings illustrates what really happens when you inject spider veins. Forget what anyone else has told you! As you now see, it's not like plastic surgery, where a skillful stroke of the knife removes the offending lump or bump. The effect of spider vein injections is to cause them to break up into smaller vessels, and to progressively thin out with successive treatments. The final panel of the drawing ("E") is the end result. This panel is intentionally drawn empty, but I must emphasize that the treated area is never really free of all visible blood vessels. If you sit under a bright light, and study the area minutely, you'll see tiny vessels, even after the treatment is over. But other people won't see them. Yet we say that after the treatment is over, the area is "clear". You may be wondering: How clear is "clear"? This is the answer: If, after the treatment is over, you stand up in front of a mirror, under normal lighting, you'll see yourself in the mirror as other people see you. You should not see any spider veins. This is the object of therapy: to get you to the point where you can walk down the street with shorts on, and not be seen by other people as having a "road map" on your legs. This result can be obtained in the great majority of cases. Another way to answer the question is this: Follow-up studies done in this office have revealed that 90% of our patients consider the treatment to have been a success, and they're glad they did it. Most of the 10% who were dissatisfied had stopped coming long before the treatment was over. In other words, if you look back to the drawing...
...the satisfied customers stuck with it until panel "E"; the dissatisfied customers quit after reaching one of the intermediate stages, usually panel "B" .Thus, after a single treatment (which is almost never enough), they lost their faith in the outcome, and are now walking about with "secondary vessels", which, in some cases, can be as unsightly as the original condition! No wonder they're dissatisfied! |
|
The injection treatment of spider veins was invented by my father, Dr. H.I. Biegeleisen, in 1934, and was published in the Journal of the American Medical Association (H.I. Biegeleisen, "Telangiectasia Associated With Varicose Veins", Journal of the A.M.A. June 23, 1934, Vol. 102:2090-2094). In spite of the fact that this is the "family business", it still took me about 5-6 years of continuous experience injecting spider veins before I developed an acceptable technique. When I hear rumors that such-and-such a doctor, who has been "in business" for a few months, claims that he can do in 1 treatment what I require 2-4 treatments to accomplish, I have to laugh. But I think it's not so funny for the patient who goes to the local amateur, spends thousands of dollars, and ends up with nothing to show for all the time and money spent. Here are the facts: When spider veins are injected, "secondary vessels" come out. Some people get more, some get less, but everybody gets some. The doctor who pursues them, and who has the technical ability and motivation to inject them with a fine needle, is the doctor who will successfully clear them. |
|
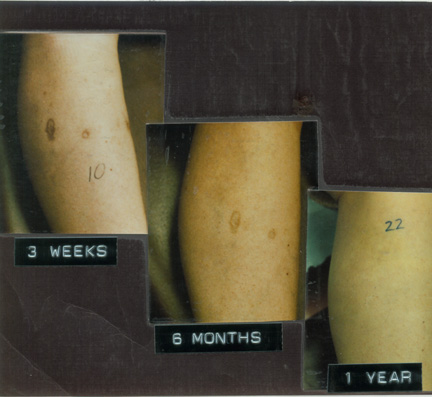
Approximately one-out-of-ten, or 10% of patients have an area somewhere on their legs which will not clear. Please don't presume that this means that the patient is dissatisfied. If the patient's leg was previously covered with veins, and only one area failed to clear, the patient will be happy indeed! When an area fails to clear, it's most frequently in the vicinity of the knee. And it is never primary vessels -- it's always secondary vessels. (The primary vessels almost always clear). The pictures below show the "before" and "after" in a case of treatment failure:
The area of treatment failure doesn't show as well on a computer screen as it does in "real life", so I've put large red arrows to draw your attention to the spot. Notice that in the photo below, the "after" photo, all the primary vessels are gone, but that a patch of secondary vessels is seen, appearing as a poorly-defined reddish blotch just above the knee. Now look at the red arrow in the photo above (the "before" photo), and note that the secondary vessels were not there before the treatment - illustrating what I said earlier, namely that the secondary vessels tend to move toward the knee. There are also patients who have more than one area which won't clear, but the numbers are much smaller (i.e., less than 10%; perhaps about 1%). In the above statement, I refer to "areas". These correspond to the groupings of vessels shown earlier:
Note again that each leg has three basic groupings, or areas, of spider veins, on the outside of the leg, and three "mirror image" areas on the inside. So there are six on each leg (i.e., twelve in all). When we speak of "an area which won't clear", we refer to one of those twelve areas. So what we're saying is that even when one area fails to clear, the other 11 areas usually do clear. It's even less likely that two areas won't clear, and the probability that none of the twelve areas will clear is almost zero. Thus, if the patient has spider veins in only one of the twelve areas, and if that one area doesn't clear, then that patient will not be happy!. But if the patient is "plastered" with unsightly spiders on both legs, from top to bottom, and if, out of all that, only one of the 12 areas fails to clear, it's not so bad! Although the cause of treatment failures is not known with certainty, it is possible to offer a very plausible explanation: the continued existence of an underlying "source" or "feeder" vessel which cannot be eradicated. Sometimes, the persistent "source" vessel is a varicose vein. If it can't be eradicated, it's either because the patient has forbid us to inject it (see our write-up on the saphenous vein to learn why people sometimes take this position), or because it's too small to get a needle into. Most of the time, however, the underlying "source" vessel which can't be eradicated is an arteriovenous communication. The reason why it won't go away is something which cannot be known with certainty, since we never see the source vessel in the first place (it's buried in the leg, somewhere below the surface; beyond what is visible, and too small to "see" on ultrasound). Why would a source vessel be stubborn like this? Perhaps because it's unusually large, or because it has unusually rapid blood flow or high pressure. Who can say? We can't see it! Whether or not an area which fails to clear looks "better" or "worse" than the original vessels is a matter of opinion. Whatever the patient's opinion is, the fact of the matter is that the area didn't clear, and doesn't look good. We never give up on such an area until we have exhausted all available remedies. To the best of my knowledge, as of the writing of this document, no patient who was ever discharged from this office with an area which we wrote off as "incurable", has gone elsewhere and gotten it "cured". Therefore, it is my opinion, as of this writing, that if we cannot clear up a particular case of spider veins, then no one else can either. When that situation changes, then this document will change also! |
|
In rare cases, a patient comes back after treatment with a more serious skin injury than the 1/4-inch blisters we have already discussed. We really do not know what causes such injuries. Clearly they result from medicine going in the wrong place. But what the place is, we don't know, and exactly how the medicine got there (i.e., what circulatory pathways it took) we don't know either. The risk of such things is surely less than 1-chance-in-1000. At the time this web site was last revised, we had not seen a serious skin injury in over 20 years. Perhaps we'll never see one again. Who can say! |
|
If you thought that anything about spider veins was simple, you know better now. Their underlying physiology is complex. Their treatment is complex. Everything about them is complex! It is, however, entirely possible to treat them. It requires multiple office visits, and many injections. These, by the way, are done with a "30-gauge" needle, which is, for all intents and purposes, the tiniest needle you can buy. Above all, it requires a skilled and dedicated operator. This is not an easy treatment, either for doctor or patient. The so-called "primary vessels", those which you have at the outset, are relatively easy to inject. But then "secondary" vessels emerge. They are tiny, and difficult to inject. Ninety percent of the time, patients are entirely satisfied with the outcome of their treatment, and they are glad to have done it. Ten percent are dissatisfied, but we have found that most of them discharged themselves, long before the treatment was over. A small percentage of patients have areas which cannot be cleared by this treatment, or by any other which we know of. In the majority of cases, however, the spider veins can be cleared from all areas of the leg. When a "cured" area is examined under normal lighting conditions, it looks perfectly clear. When examined very closely, under a bright light, tiny vessels will be seen. No leg can be made 100% "physiologically clear" of spider veins. But a good cosmetic clearing is the usual result. There are no medically-significant side-effects to this treatment. But there are minor cosmetic side effects in 1-2% of cases. In about 1-out-of-1000 cases, a more significant skin injury occurs, which leaves a scar. This concludes our introduction to spider veins! If you have any further questions, ask us at your consultation. But don't be surprised if we don't know the answers! If you've studied this brochure carefully, then you know almost as much about spider veins as we do! |
|
|
Ken Biegeleisen, M.D. 212-717-4422 |
|
CLICK "BACK" TO RETURN |