|
|
The complete history of the A justifiable diatribe by Ken Biegeleisen, M.D., Ph.D.
|
|
|
|
The complete history of the A justifiable diatribe by Ken Biegeleisen, M.D., Ph.D.
|
|
|
|
Introduction
I was the son of America's foremost proponent of the treatment of varicose veins by injection, i.e., by non-surgical means. On the other hand, the surgeons of the early 20th century were dead-set against any primary vein therapy which did involve an operation. I shall not review the entire tortuous history of the 20th century "injections vs. surgery" war here, but only reveal the outcome. By the latter end of the century, it had emerged that both injections and surgery had advantages and disadvantages. The primary advantage of injections was that the outcome looked better, which was important in a field which is primarily cosmetic. The superior cosmetic outcome did not necessarily prove, however, that the injection method itself was superior, but merely that injections could be repeated until the desired outcome was achieved. In contrast, however, you couldn't take the patient back to the operating room over and over again, and even if some aggressive surgeon had proposed to do so, no patient would have consented. |
|
|
|
The advantage of surgery was that the remission time, on the average, was longer. I said "remission", and not "cure", because it has been known for 50 years that you can't cure varicose veins. Given time, they always grow back. So we can speak only of "remission", not "cure". In the majority of cases of varicose veins, the differences in long-term remission time between surgery and injections are not all that large, but they are large enough to be "statistically significant". On the other hand, in a minority of cases, the differences can be large indeed. When I entered the venous field, I decided to set out to find a better way. I began this endeavor by sitting down and asking myself a question: "What would be the characteristics of the ideal sclerosant"? A "sclerosant", by the way, is a medicine used for the injection treatment of varicose veins. |
|
|
|
Ideal sclerosant found! The job of a sclerosant is that it must shut a vein down, especially in key anatomic spots where abnormal blood flow is known to arise. Thus, the characteristics I perceived to be important for the development of an ideal sclerosant were (1) that it fix itself, like an adhesive, in the key anatomic spots requiring closure, (2) that it not be readily dislodged from that spot, (3) that it not be quickly resorbed by the body, but (4) that it should ultimately dissolve, so there would be no question of long-term implant reactions. I soon realized that the place to seek this substance would be in the annals of invasive radiology, where doctors were using fluoroscopy to place occlusive substances into vascular cancers in the brain; an organ into which surgeons cut only with great reluctance. The substances in use at that time (the early 1980's) included ethanol, gelfoam and tiny steel coils, but according to the textbooks, the embolic agent of choice was Bucrylate, the trade name for 2-isobutylcyanoacrylate. Bucrylate had all the necessary chemical/physical properties required for an ideal sclerosant, and was additionally attractive in that it had already been tested in the venous system. A Belgian radiologist named Marc Kunnen was using Bucrylate to treat "varicocele", a varicosity of the Internal Spermatic Vein of the scrotum, which originates in the pelvis at the level of the renal vein (Kunnen & Comhaire, Annals of Radiology, 27:303, 1984). Kunnen was threading a catheter up to the origin of the varicocele under fluoroscopy, then injecting Bucrylate, with excellent results. Upon learning of Kunnen's activities, I immediately invited him to the United States to lecture to our Phlebology Society of America annual Congress, thinking that the American phlebological community would jump at the chance to learn of a new and apparently near-perfect sclerosant. I was wrong. There was no interest at all -- except, that is, for my interest. I made up my mind to try Bucrylate in leg varicosities as soon as possible. |
|
|
|
Bucrylate can be thought of as an overpriced, ultra-purified medical grade of Krazy Glue. It was manufactured by Permabond, a subsidiary of Eastman Kodak, and sold by Ethicon, a subsidiary of Johnson & Johnson. In those "pre-9/11" days, ordering research chemicals was relatively easy, because everyone ordering chemicals was not automatically classified as a "terrorist", and people were not hiding under their desks in fear of quasi-imaginary "enemies". Thus, I soon found myself in the possession of a box of ampuoles of the new wonder drug. I tried Bucrylate in a few veins, starting with my own. Here's what I learned. The substance polymerizes instantly when it encounters blood. Therefore, it is best injected via butterfly needle, with 0.5 cc of saline in the tubing in front of the glue, for if the glue extends all the way to the tip of the needle at the moment the vein is cannulated, the needle will become totally occluded by polymerization before the injection is made. I learned further that the amount of Bucrylate necessary to permanently occlude a vein is too small to measure, because even in cases where the plunger of the syringe froze immediately, indicating premature polymerization of the glue at the needle tip, the vein closed down and never re-opened. The word "permanent", as used here, is correct. I have, in my own body, three veins which were injected with Bucrylate over 20 years ago, and they remain closed to this date. In two severe varicose veins which I also treated, the same holds true. That is, even though there has been substantial recurrence around the Bucrylate blockages since that time, the injected segments of vein remain occluded over 20 year later. We thus learn that Bucrylate is pretty close to being an ideal sclerosant. The trouble with Bucrylate is that it is too darned good. A medicine which can permanently close a blood vessel after injection of a single drop is certainly not something one wants to inject casually into the circulatory system, with no thought of consequences. I knew, from my review of the medical literature on bad injections into the Saphenous Vein, that an accidental injection into the adjacent Femoral Vein, with "traditional" sclerosants, was usually harmless, and that even an accidental injection into the Femoral Artery usually caused only transient swelling, and not permament tissue damage. But now I was considering Bucrylate injection into these same vessels, and the prospects for devastating vascular and tissue damage were frightening. |
|
|
|
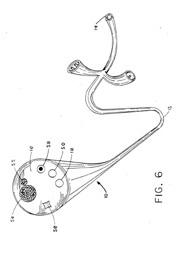
New delivery system devised for Bucrylate It was at that moment that I conceived of the Venoscope. What I envisioned was a fiberoptic catheter with an injection channel, through which the injection could be made under direct vision. This, I postulated, would make it possible to verify the injection site with absolute certainty, so that the possibility of accidental injection into the Femoral Artery or Vein could be eliminated entirely. There still remained, however, the possibility that the Bucrylate, once injected, might migrate upwards into the Femoral Vein before adhering to the Saphenous Vein wall. I knew that migration of the Bucrylate downward would be harmless, but migration upward might be disastrous. Whether Bucrylate would migrate at all, and whether, if it did, it went up or down, would be determined entirely by the direction and velocity of blood flow at the instant of injection. We thus had to obtain that information, since both parameters, namely direction and velocity of blood flow, were notoriously variable in the Saphenous Vein. Therefore, it would be essential that the Venoscope have doppler capabilities. It happens that pure fiberoptic "angioscopes" with injection channels already existed, and were being widely used by vascular surgeons for various applications. Pure doppler catheters also existed, and although not widely used, they were held, by their proponents, to be the equivalent of iodine-contrast angiography in coronary catherization studies. So what I was thinking of was to combine these two pre-existing technologies in a single instrument. Once I had begun thinking of a new instrument, I endeavored to impart to it all capabilities possible with the technologies embedded into it. If, instead of inserting a single piezoelectric crystal for doppler flow studies, we inserted an array of crystals, we could do ultrasound imaging, which would be immensely valuable in areas of the circulation having brisk blood flow. You see, it is highly-desirable to work under direct fiberoptic vision, but that requires an infusion of clear fluid (such as saline) into the vein, because you can't see through blood. In many cases, working thusly under direct vision is quite possible, but at certain key locations in the venous system, the blood flow is too rapid to wash out with a saline infusion, unless the infusion is so rapid that it poses a risk of pulmonary edema (even 500 cc of liquid infused rapidly into the circulatory system can cause death in the elderly or sick). It is in these areas that ultrasound imaging, which would be ultra-clear from within the vessel, would be a blessing. Finally, the Venoscope, in order to be a true medical step forward, would have to be steerable. This attribute also existed in catheters current at that time. The steerability would make possible the super-selective ablation of either proximal Saphenous tributaries or arteriovenous communications. The uses of the Venoscope which I envisioned were:
The treatments I envisioned included:
Of these three methods, I considered "laser" to be the least useful, although anything "laser" has been most marketable to a dumbed-down medical profession and general public. This notwithstanding, I added "laser" to my patent application, just for completeness. But was laser treatment of varicose veins even possible? No one knew! What would happen when you switched on a million-degree light beam in a blood vessel filled with blood? Clearly, there would be boiling. What would happen to the steam? Clearly there would be charred tissue. What would happen to the charcoal? No one knew the answers to any of these and other quesitions. Furthermore, the "diode lasers" used in the new laser-burning vein devices weren't available at that time. The closest thing to a practical intravascular laser was the IBM excimer laser, which was being used in opthalmologic applications, and which was reputed to work in an aqueous environment. Buoyed by this information, I pursued the matter further. I learned later of the work of a man named Roman Nowygrod, a research vascular surgeon at Columbia University, who was studying vein grafts in arterial bypass surgery of the legs. Nowygrod had been working on new ways to fasten small pieces of vein together, end-to-end. "Traditionally", this was done by suturing, a tedious and time-consuming task. In other words, if a single, sufficiently-long vein graft could not be found in the patient's body, two or more smaller grafts would be lined up and sewed together under the operating microscope, right in the operating room, while the patient lay on the table under general anesthesia. In order to cut down on anesthesia time, Nowygrod wanted to perform the anastomosis using laser, to obtain a "weld", which, he reasoned, could be done in a fraction of the time necessary to sew the same vessels together under the microscope. His initial welds were pressure-tested, and held up to 200 mmHg, which exceeds anything required for the venous system, but not the arterial system. He then painted the anastomotic sites with fibrinogen and a chromophore (fluorescein isothiocyanate), which caused the strength of the laser welds to increase to 400 mmHg, exceeding even the highest pressures ever seen in the arterial system. Clearly, laser welding of veins was possible. But still, Nowygrod was doing his welds outside the body, on the operating room table, and many questions about the use of laser inside a living vein remained. I went to visit Nowygrod at Columbia, and tried to interest him in pursuing venous work. He was not interested. |
|
|
|
Patenting, marketing and expropriation of the Venoscope In 1989 I had applied for, and in 1991 I was granted U.S. Patent # 5,022,399 for the Venoscope. Frankly, I was surprised that the Patent Office granted it, since I had prior experience with them, and knew that they could be extremely difficult to deal with. But, for whatever reason, they approved this patent application after only two years of arguments. I then embarked on a program to sell the Venoscope concept to industry. I approached dozens of companies, including the fiberoptic giants (Olympus and Baxter) and all the lesser manufacturers (including but not limited to the following: Schott, Medscan, Eli Lilly, GV Medical, Intramed, United States Surgical, Valleylab/Pfizer, Circon/ACMI, Cardiovascular Imaging Systems, ET Medical Systems, BTG International, and, later, Diomed and Angiodynamics). No one wanted to have anything to do with the Venoscope, the typical rejection letter reading something like this: "This invention is not needed -- our consultants inform us that existing remedies are adequate". Really? Then how come my invention is now in every hospital in the United States, and I get no royalties? But I'm getting ahead of myself. In 2001, I got a call from my mother-in-law, informing me that a doctor was talking about "laser treatment of varicose veins" on television. I turned on my TV, and quickly located the report. It was a primitive device, to say the least. Although it was fiberoptic-based, it couldn't even see into the vein. The optical fibers were there solely for burning. It had no doppler capabilities (i.e., it was, in a manner of speaking, "deaf"), no injection channel, and no mechanism for steering. It was good for nothing except blindly cannulating a huge varicose vein, and burning the living daylights out of it. This would produce a result which would be predicted to be the equivalent of bad surgery, since it brutalized the vein without even the possibility of attending to the fine points of anatomy necessary to complete a properly-performed operation. Yet, almost from the start, spin masters were duplicitously proclaiming the new laser to be "the equivalent of surgery" (i.e., "good" surgery), and to be capable of bringing about "permanent cures". In other words, people were lying like hell. The man giving the TV interview was one Robert Minn, a name I did not know. He was said to be on the faculty of New York Hospital/Cornell Medical Center. I called him immediately. Do not think for a moment that I accused him of anything. The thought that he had "stolen" my invention never once entered my mind at that time, because his device seemed far too primitive to have been derived from the Venoscope. The purpose of my call, rather, was to propose that we collaborate. Toward this end, I first congratulated him on his good work, then tried to explain to him that his device only scratched the surface of what was possible with such catheter-based technology. To my surprise, he responded to my proposal not with a "yes", or a "no", or even with a "maybe", but rather with mysterious words to the effect that "I would have to speak with his liason at 'the company' ". Strange... It sounded like I was dealing with a futuristic sci-fi movie super-villian of some sort; a huge company which operated in the shadows, interacting with the public through non-empowered spokesmen. Be that as it may, I obeyed Minn's orders, and contacted his "liason" at the company, who turned out to be not an officer, but a salesman named Tony Jacobowsky. All Jacobowsky told me, however, was that he would take the matter up with his "superiors" at...The Company. Then, he said, he would get back to me. But he never did get back to me. Subsequently, I wrote, telephoned, and emailed "The Company" directly, but I never once got back so much as a 1-line reply. I never even received a courtesy form-letter acknowledging that I had written. Nevertheless I still, at that early juncture, was too naive to suspect patent infringement, and I put the matter on the back burner, pending further developments. I presumed, I think now perhaps wrongly, that there were no significant sales yet, and the thought of a lawsuit was far from my mind. At that time (2001), I had already been enthusiastically promoting Venoscopy for twelve years. As soon as my patent application had been submitted (1989), I had immediately launched into a program of educational lectures and writings. Here are the six most prominent of those: Biegeleisen K. Use of a Specially Modified Angioscope for Accurate Injection of Sites of Deep-to-Superficial Reflux in Varicose Veins. In: Proceedings of the 12th Annual Congress of the Phlebology Society of America, pp. 42-51. Published by the Phlebology Society of America, 5530 Wisconsin Avenue, NW, Washington, DC 20815. (Based on a presentation at the 12th Congress, May 18-20, 1989, Hyatt Regency Hotel, Kansas City, Missouri). Biegeleisen K. Use of the Venoscope for the Treatment of Varicose Veins. Presented at the 10th World Congress of Phlebology, Strasbourg, France, September 25-29, 1989. Published in Phlebology 89 (Actes du 10e Congrés Mondial, Union Internationale de Phlébologie), John Libbey Co., Ltd., London, 1989, pp. 419-422. Biegeleisen K. Venoscopy: A Useful Adjunct in Treating Varicose Veins. Proceedings of the 13th Annual Congress of the Phlebology Society of America. Published by the Phlebology Society of America, 5530 Wisconsin Avenue, NW, Washington, DC 20815. (Based on a presentation at the 12th Congress, May 10-12, 1990, Drake Hotel, Chicago, Illinois). Biegeleisen K. Venoscopy (venous angioscopy) as an adjunct to the surgical and non-surgical treatment of varicose veins. Phlébologie 92 (Proceedings of the XIth World Congress of the International Union of Phlebology, Palais des Congrés, Montréal, Canada, August 30-September 4, 1992), Eds. P. Raymond-Martimbeau, R. Prescott, M. Zummo. John Libbey Eurotext, paris, 1992, pp. 677-679. Biegeleisen K & Nielsen RD. Failure of angioscopically-guided sclerotherapy to permanently obliterate greater saphenous varicosity. Phlebology, 1994, 9:21-24. Biegeleisen K. Macrosclerotherapy and angioscopy. Chapter in: Ambulatory Treatment of Venous Disease. Ed. Goldman MP, Bergan JJ. Mosby, St. Louis, MO., 1995, pp. 135-140.
The Venoscope concept had thus been revealed and discussed at two American Congresses of Phlebology, three World Congresses of Phlebology, one stringently peer-reviewed vascular journal (Phlebology), and a widely-read textbook edited by two of the most prominent figures in the venous field (Goldman and Bergan). I should note that at the 1989 World Congress (reference #2 above) I showed the world's first intravascular video of a prototype venoscopic therapy, namely a case of angioscopic sclerotherapy. Even to this day, this remains the most sophisticated venous therapeutic procedure which has been reported upon, since the field of Phlebology has only devolved since then. It can thus be said, with certainty, that no one of any standing in the venous field can possibly have been unaware that Venoscopy was coming. It was only a question of when. And come it did! But -- if we are to accept outward appearances -- apparently not from me. And not in the technologically-advanced form I had intended, but rather in the form of a backward-looking, stripped-down cheap marketing gimmick. I refer, of course, to the blind, deaf and dumb vein-burning catheter featured in the TV promotion mentioned above. It was not until some years later that I realized who was the apparent "mastermind" behind this dumb but lucrative new invention. It was none other than Luis Navarro, one of New York City's most commercially-successful vein entrepreneurs. I was quite surprised, although I knew well of Navarro's earlier marketing activities. Around 1980, I launched the nation's first successful advertising campaign for non-surgical treatment of varicose veins (which, by the way, I am no longer proud of now) -- during a period when the medical profession was still very unsure about the propriety of medical advertising. Very shortly thereafter, Dr. Navarro launched his own advertising campaign, becoming the nation's second major vein advertiser. Draw your own conclusions. When I hired a public relations man, becoming almost surely the first doctor to do a television story on non-surgical treatment of varicose veins (another "first" I'm not particularly proud of now), Navarro did likewise, becoming the second. Draw your own conclusions. When I moved my office to 64th Street on New York City's east side, Navarro shortly afterwards moved his office to east 65th Street. Coincidence? Who can say? One day, a female patient with an accompanying man came to my office for a consultation, and my secretary recognized the accompanying man as none other than Luis Navarro himself. He did not announce himself, and had my secretary not recognized him, his visit would have gone un-noticed. What was he doing there? Draw your own conclusions. In 1999, ten years after my Venoscope patent was filed with the U.S. Patent and Trademark Office, Luis Navarro and several collaborators (including Robert Minn) were granted a patent for their blind, deaf and dumb vein-burning laser catheter. It is said that "imitation is the sincerest form of flattery", and, I assure you, I'm most flattered. But where's the credit? The law requires that all "prior art" be acknowledged in a patent application. I'm not mentioned at all in the Navarro patent! Is it possible that Navarro et al came up with the idea independently? Not likely. I've already listed my publications and presentations above. No one of even the slightest stature in the venous field can possibly have been totally unaware of this new approach, especially since I was not the only person discussing it (although I was, to the best of my knowledge, the only one to patent a fibroscopic catheter for venous work). Besides, one of the co-authors of the Navarro patent, Carlos Salat, had referenced my work in his own prior writings. It is thus established that they knew of my work. Their choice to pretend that I didn't exist was thus quite deliberate. |
|
|
|
The fox guarding the hens gets out-foxed At the same time that all this was happening, I learned that a second company, called Angiodynamics, had marketed yet another blind, deaf and dumb catheter, and that Diomed had immediately sued, alleging that Angiodynamics had stolen their idea! In New York, this is called "chutzpah". I managed to obtain copies of the paperwork submitted by both sides in this ridiculous court battle. Angiodynamics' reply to Diomed's complaint might surprise you. They claimed that neither of their patents was valid, because neither one referenced "The Biegeleisen Paper" (one of my 1989 papers; #2 in my list of publications above) as prior art! If you have nothing better to do, you can click here to read the entire Angiodynamics defense. Alternatively, just click here to see pages 10-11 of their defense, where the references to my work are highlighted, culminating in Angiodynamics' claim that Diomed committed "inequitable conduct or fraud" by withholding knowledge of my work from the Patent Office.
Sounds like I have an air-tight case of patent infringement, does it not? If you thought so, guess again. Both these parties believe that by taking things out of the Venoscope, they have turned it into a "new" invention. Specifically... This leaves a blind, deaf and dumb catheter which does nothing but indiscriminately burn blood vessels. Is this what you call a "new" invention? Or is it merely the expropriation of pre-existing good technology for the purpose of cashing in on a stripped-down, cheap marketing gimmick? I must not say; you'll have to decide for yourself. |
|
|
|
And what did the court think about all this? In an interim decision written by Judge Nathaniel Gorton, the festering corruption in the court was well-illustrated by language which was shamelessly obfuscated for the evident purpose of providing a lame excuse to grant "judgment" to the plaintiff. Was the judge merely stupid? Was he too tired to take the case seriously? Or did he receive a gift to "blind the eyes" (Deuteronomy 16:19)? You decide. Here's what he said, in dismissing me as "prior art": "...a 1989 article by Biegeleisen...did not anticipate the '777 patent (i.e., the Diomed patent) because Biegeleisen's process entails use of an angioscope with a crystal tip rather than a laser. Furthermore, plaintiff (i.e., Diomed) contends that the article fails to disclose direct contact with the vessel wall, compression, drainage or any decrease in vessel diameter." I would dismiss these comments as frivolous assininity, except that they have diverted hundreds of millions of dollars to people who have no interest in the health of patients, or in the advancement of medicine. In doing so, they have also established a thus-far impassable block to progress, since they create a huge incentive to cash in on hype and corruption, rather than to risk venture capital on legitimate research. (The entire interim decision can be read by clicking here, or, alternatively, the page quoted above can be quickly accessed by clicking here.) |
|
|
|
In case it's not perfectly obvious, the judge's dismissal of my prior art, by referring to it as an "angioscope with a crystal tip rather than a laser", is meaningless techno-babble, meant solely to deceive the ignorant. There's no such thing as a "crystal tip", and even if there was, Diomed's angioscope doesn't have a laser in it anyway. These words are only there for the purpose of creating an excuse to give Diomed money they don't deserve. The other comments, such as "direct contact with the vessel wall", are a total joke. Every catheter which has ever been inserted into a blood vessel since the World began made "direct contact with the vessel wall". Who the hell do they thing they're fooling? And what's this about "drainage"? The Diomed catheter has no channels, it can't drain anything. How about "Decrease in vessel diameter"? What's that? Every non-surgical treatment of varicose veins is designed to decrease the vessel diameter. Diomed's method is no better than a half-dozen prior methods which are just as effective or more so. This is all obfuscation. The trouble is, the obfuscation worked, because the court granted "judgment", or the appearance of judgment, to Diomed, and ordered Angiodynamics to pay millions of dollars in "damages". Poor Diomed was "damaged", boo-hoo. If Diomed was so damned proprietary, then why are there now a slew of companies making blind laser-burning venous catheters, each new one more pointless than the last? Here's a short list of companies currently cashing in on Venoscope knock-offs: Diomed Not one of these lying companies, by the way, has granted me the courtesy of a reply to any of the correspondence I sent them. I apparently don't exist, as far as they're concerned. Only people with lots of money exist. The rest of us are merely here to be plundered by them. Finally, and most importantly, we must ask why does the insurance industry pay more for these idiotic laser treatments than for legitimate surgery? And who are all the so-called "researchers" writing that laser is the "equivalent" of surgery, which they know is a damned lie? If the only issue here was "my" royalties, then the present diatribe would have no merit. But it does have merit. In the words of Ghandi, it "makes the injustice visible". The true victim of all this thievery and expropriation is you, and all other patients with vein disease, who naively assume that the medical establishment is laboring to advance medicine on their behalf. That's simply not true! The medical establishment, at least this segment of it, is laboring to steal as much money as it can get its hands on, endeavoring to do not a stitch of work more than absolutely necessary to avoid the appearance of impropriety. Even they have enough common sense to realize that they should avoid appearing so vastly dishonest, that even the layman will see through their schemes. |
|
|
Ken Biegeleisen, M.D. 212-717-4422 |
--CLICK "BACK" TO RETURN--
--OR--